From May 29 to June 2, the highly anticipated 2026 Annual Meeting of the American Society of Clinical Oncology (ASCO) was held in Chicago, United States. Among the many highlights presented at the conference, bispecific and trispecific antibodies targeting CD3 and PD-1 attracted particular attention.
PD-1 Bispecific Antibodies Enter the Commercial Validation Phase
Ivonescimab
HARMONi-6 (AK112-306), a pivotal Phase III head-to-head study of ivonescimab, directly compares it with the current standard PD-1 monoclonal antibody regimen, tislelizumab in combination with chemotherapy. It is one of the few randomized Phase III trials to date conducted in the context of standard immunotherapy-based combination therapy that evaluates a mechanism upgrade strategy.
From a study design perspective, the key significance of this trial lies in the fact that it is not intended to demonstrate whether immunotherapy works in general. Instead, it directly evaluates whether adding VEGF targeting to an established PD-1 backbone can further improve survival outcomes. As such, the study should be fundamentally understood as a structural upgrade comparison within the PD-1 treatment platform, rather than a cross-mechanism comparison between immunotherapy and non-immunotherapy approaches.
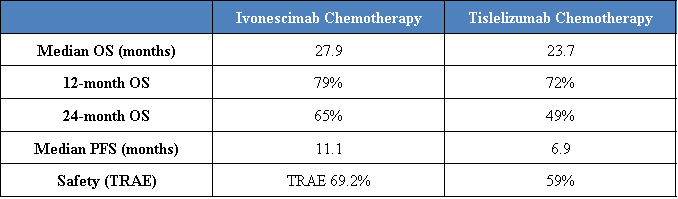
The results demonstrate that, in a head-to-head setting against the standard PD-1 plus chemotherapy regimen, the PD-1 VEGF bispecific antibody achieved consistent benefits across both overall survival and progression-free survival, with a trend toward progressive separation of survival curves over long-term follow-up. This pattern suggests that the observed benefit may not be limited to early tumor control enhancement, but could also be associated with sustained remodeling of the tumor microenvironment.
Against the backdrop of a maturing PD-1 PD-L1 landscape and diminishing marginal returns from further incremental improvements, the key implication of these findings is that this represents one of the first randomized Phase III head-to-head datasets to demonstrate improved overall survival beyond a standard PD-1 based regimen. This positions PD-1 VEGF bispecific antibodies as a leading candidate within the next-generation immuno-oncology upgrade pathway.
However, the current OS data should still be considered as an interim analysis and will require further validation with longer follow-up. In addition, as the study is primarily based on a Chinese patient population, its global generalizability remains to be further confirmed in subsequent studies.
PF-08634404
PF-08634404 (SSGJ-707), a Phase II study of a PD-1/VEGF bispecific antibody in previously untreated advanced NSCLC, further evaluates the clinical activity of dual PD-1 and VEGF blockade in a patient population currently treated with PD-1-based standard-of-care regimens. In previously untreated patients with advanced NSCLC who were driver mutation-negative and had PD-L1 TPS ≥1%, PF-08634404 monotherapy demonstrated notable antitumor activity. In the 10 mg/kg Q3W cohort, the confirmed objective response rate (ORR) reached 67.6%, while median progression-free survival (PFS) was 12.4 months. Median duration of response (DOR) and overall survival (OS) had not yet been reached at the time of analysis, indicating both a high level of initial tumor response and the potential for sustained clinical benefit. Importantly, these outcomes were achieved without the addition of chemotherapy, further supporting the therapeutic potential of dual PD-1 and VEGF blockade as a monotherapy approach.
From a strategic perspective, the significance of this study extends beyond the reported efficacy outcomes. Rather than serving solely as a validation of an individual product, the findings provide further evidence supporting the reproducibility of the PD-1/VEGF bispecific antibody mechanism across different molecules. Ivonescimab has previously established the clinical relevance of this approach in NSCLC through the HARMONi program. The observation of similarly encouraging efficacy signals with PF-08634404 in a comparable patient population suggests that the field is progressing from validation of a single leading asset toward broader validation of the underlying therapeutic platform.
As a global program under Pfizer's leadership, PF-08634404 reflects growing interest among multinational pharmaceutical companies in the PD-1/VEGF bispecific antibody space and underscores increasing confidence in the biological and clinical rationale of this therapeutic strategy. As global Phase III development programs continue to advance, PD-1/VEGF bispecific antibodies are increasingly emerging as a significant area of competition within the next generation of immuno-oncology therapies.
Nevertheless, the current results are derived from a Phase II study and remain preliminary. Longer follow-up and subsequent randomized trials will be required to fully characterize the durability of benefit and confirm the clinical impact of this approach across broader patient populations and global treatment settings.
Volrustomig
Volrustomig, a PD-1/CTLA-4 bispecific antibody developed by AstraZeneca, is designed to preferentially enhance CTLA-4 blockade on PD-1-positive activated T cells, with the aim of improving antitumor efficacy while mitigating the toxicity traditionally associated with dual immune checkpoint inhibition. The eVOLVE-02 study evaluated its activity as monotherapy in patients with recurrent or metastatic head and neck squamous cell carcinoma (R/M HNSCC).
Among patients with PD-L1 CPS ≥1, volrustomig achieved a confirmed objective response rate (ORR) of 26.3% and a disease control rate (DCR) of 52.6%. Notably, 60% of responders remained in response at the time of data cutoff. Although the study was limited by a relatively small sample size and short follow-up duration, the results demonstrated encouraging antitumor activity. In addition, the incidence of grade 3/4 treatment-related adverse events was 8.7%, with no treatment discontinuations due to toxicity, supporting a favorable safety profile.
This study extends beyond the reported ORR. Rather, it provides additional clinical validation for PD-1/CTLA-4 bispecific antibodies as a next-generation immune checkpoint intensification strategy. As the clinical benefit achievable with PD-1 monotherapy approaches a plateau in multiple tumor types, the precision dual checkpoint blockade approach represented by volrustomig is emerging as an important direction for immuno-oncology innovation in the post-PD-1 era.
CD3 Bispecific and Trispecific Antibodies Continue Their Expansion into Solid Tumors
Alveltamig
Alveltamig (ZG006) is a DLL3/DLL3/CD3 trispecific T-cell engager (Tri-TCE) designed to simultaneously bind two distinct DLL3 epitopes on tumor cells and CD3 on T cells, thereby facilitating precise T-cell recruitment to the tumor microenvironment and promoting targeted tumor cell killing. The ZG006-003 study was conducted to optimize dosing and evaluate the efficacy and safety of alveltamig in patients with previously treated neuroendocrine carcinoma (NEC).
From an efficacy perspective, Alveltamig demonstrated a clear dose-response relationship. In the 30 mg cohort, the confirmed objective response rate (ORR) reached 37.5%, with a disease control rate (DCR) of 62.5%, both exceeding those observed in the 10 mg cohort. Particularly noteworthy were the results in patients with high DLL3 expression (≥50%), where the 30 mg dose achieved an ORR of 56.3% and a DCR of 75%. Median progression-free survival (PFS) in this subgroup reached 8.41 months, compared with 3.02 months in the corresponding 10 mg cohort. These findings suggest that DLL3 may serve not only as a therapeutic target but also as a potentially valuable predictive biomarker for patient selection.
The safety profile was generally consistent with expectations for T-cell engager therapies. Although treatment-related adverse events were reported in all patients, the majority of cytokine release syndrome (CRS) events were grade 1 or 2 in severity. Only a limited number of grade 3 CRS events were observed, all of which were manageable, and no grade 5 treatment-related adverse events were reported.
This study provides a further validation of DLL3 as a key therapeutic target in neuroendocrine malignancies. In recent years, DLL3 has emerged as one of the most actively pursued targets for T-cell engager development in small cell lung cancer and neuroendocrine tumors. By incorporating a dual-DLL3 epitope binding design, alveltamig is intended to enhance tumor binding avidity and improve immune synapse formation, potentially translating into greater antitumor activity. The observation of an ORR exceeding 50% and substantially prolonged PFS in DLL3-high, previously treated NEC patients, a population with significant unmet medical need, represents an important clinical validation of the DLL3-targeted trispecific antibody approach.
QLS31905
QLS31905, a Claudin18.2/CD3 bispecific antibody developed by Qilu Pharmaceutical, is designed to redirect T cells toward Claudin18.2-expressing tumor cells, thereby enabling targeted tumor cell killing. This study evaluated the efficacy and safety of QLS31905 in combination with chemotherapy as a first-line treatment for patients with Claudin18.2-positive pancreatic cancer (PC) and gastric cancer (GC).
From an efficacy perspective, QLS31905 demonstrated substantial antitumor activity across both tumor types. In the pancreatic cancer cohort, the objective response rate (ORR) reached 59.8%, with a disease control rate (DCR) of 89.0%, a median progression-free survival (PFS) of 8.74 months, and a median overall survival (OS) of 15.87 months. In the gastric cancer cohort, efficacy outcomes were even more pronounced, with an ORR of 74.4%, a DCR of 93.0%, and a median PFS of 10.09 months. Notably, meaningful clinical responses and durable benefit were also observed in patients with low Claudin18.2 expression, suggesting that the activity of QLS31905 may be less dependent on target expression levels than some previously developed Claudin18.2-directed therapies. From a safety standpoint, the maximum tolerated dose (MTD) was not reached, and no QLS31905-related deaths were reported, indicating a manageable safety profile.
This study provides further validation of Claudin18.2 as a promising target for T-cell engager development in solid tumors. Previous successes in the Claudin18.2 field have largely been driven by monoclonal antibodies and antibody-drug conjugates (ADCs), whereas QLS31905 represents a T-cell redirection strategy that combines Claudin18.2 targeting with CD3-mediated T-cell engagement. The results are particularly noteworthy in pancreatic cancer, a disease characterized by substantial unmet medical need and historically limited responsiveness to immunotherapy. In this context, an ORR approaching 60% and a median OS nearing 16 months represent highly encouraging clinical outcomes.
From a broader competitive perspective, while DLL3-targeted bispecific and trispecific T-cell engagers have primarily focused on neuroendocrine malignancies, QLS31905 extends the T-cell engager paradigm into high-incidence gastrointestinal cancers such as gastric and pancreatic cancer. These findings suggest that T-cell redirection strategies are continuing to expand beyond hematologic malignancies into a wider range of solid tumors. As development in this area accelerates, Claudin18.2 is increasingly emerging as one of the most important solid tumor T-cell engager targets, with the potential to become a major focus of next-generation immuno-oncology innovation alongside DLL3.
Conclusion
The bispecific and trispecific antibody data presented at ASCO 2026 highlight two of the most important directions currently shaping the immuno-oncology landscape.
On one hand, PD-1-based bispecific antibodies are entering a commercial validation phase. The positive Phase III results from ivonescimab and the encouraging Phase II data from PF-08634404 provide growing evidence that mechanism-enhanced immunotherapies may deliver meaningful clinical improvements beyond established PD-1 treatment paradigms. Rather than competing with conventional immunotherapy, these agents seek to optimize and extend the PD-1 platform through complementary biological pathways such as VEGF and CTLA-4, positioning them as leading candidates for the next generation of immune checkpoint therapies.
On the other hand, CD3-based bispecific and trispecific antibodies are demonstrating increasing potential to expand beyond hematologic malignancies into solid tumors. The encouraging results reported for alveltamig in neuroendocrine carcinoma and QLS31905 in gastric and pancreatic cancers suggest that T-cell redirection strategies are beginning to overcome some of the historical challenges associated with solid tumor treatment. At the same time, targets such as DLL3 and Claudin18.2 are emerging as important platforms for future T-cell engager development.
Taken together, the data presented at ASCO 2026 suggest that the field is entering a new phase of evolution. While the first generation of immunotherapies established immune checkpoint inhibition as a standard treatment modality, the next wave of innovation appears increasingly focused on enhancing therapeutic efficacy through multispecific antibody engineering. Whether through dual checkpoint modulation, simultaneous targeting of immune and tumor microenvironment pathways, or direct T-cell redirection, bispecific and trispecific antibodies are rapidly becoming a central driver of innovation and competition in global immuno-oncology.